
The influence of melatonin and agomelatine on urodynamic parameters in experimental overactive bladder model – preliminary results
Łukasz Dobrek 1 , Piotr Thor 1Streszczenie
Wstęp: Nadaktywny pęcherz moczowy (overactive bladder; OAB) jest chorobą o złożonej patogenezie, obejmującej mechanizmy neurogenne, miogenne oraz zmienioną aktywność parakrynną urotelium. Celem naszej pracy było ocenienie czynności pęcherza, rejestrowanej w badaniach urodynamicznych, w doświadczalnym modelu ostrego (AOAB) i przewlekłego (COAB) pęcherza nadaktywnego wywołanego cyklofosfamidem (CYP), w odpowiedzi na podanie melatoniny (MLT; antyoksydant i agonista receptorów MT) lub agomelatyny (AMT; agonista receptorów MT oraz antagonista receptorów 5HT2C).
Materiał/Metody: Badania prowadzono w siedmiu grupach: 1 – kontrolna, 2-4 – grupy, w których badano wpływ MLT w obydwu modelach (AOAB i COAB) oraz grupy 5-7, w których oceniano wpływ AMT, analogicznie w dwóch modelach (AOAB i COAB). U każdego ze szczurów w znieczuleniu uretanowym wykonano wyjściowy zapis urodynamiczny oraz po podaniu 50 (grupa 2 lub 5), 75 (grupa 3 lub lub 6) oraz 100 mg/kg m.c. (grupy 4 lub 7) melatoniny (w grupach 2-4) lub agomelatyny (w grupach 5-7), oceniając klasyczne parametry urodynamiczne.
Wyniki: Zarówno MLT, jak i AMT nie wpływały znacząco na wartości parametrów urodynamicznych u szczurów z AOAB. W modelu COAB, po podaniu 75 i 100 mg/kg m.c. MLT obserwowaliśmy poprawę zapisu urodynamicznego. AMT w dawkach 75 i 100 mg/kg m.c. powodowała zaburzenia w zapisach sugerujące nasilenie nadaktywności pęcherza.
Dyskusja: Uogólniając, melatonina zmniejszała nadaktywność pęcherza w modelu COAB wywołanym CYP. Agomelatyna, w przeciwieństwie do melatoniny, nasilała dysfunkcję pęcherza w tej grupie. Wyniki te sugerują, iż obserwowana poprawa parametrów urodynamicznych po melatoninie może wynikać z jej właściwości antyoksydacyjnych a nie z aktywacji receptorów MT. Jednak niekorzystny wpływ agomelatyny na czynność pęcherza w COAB może być wynikiem nie tyle aktywacji receptorów MT bez towarzyszącego działania antyoksydacyjnego, ale wynikać ze współistniejącego efektu antagonistycznego w stosunku do receptorów 5HT2C.
Summary
Introduction: Overactive bladder (OAB) is a common disease entity with complex pathogenesis that involves neurogenic, myogenic and abnormal paracrine urothelial activity mechanisms. Our objective was to estimate bladder functioning in urodynamic studies in experimental, both acute (AOAB) and chronic (COAB) cyclophosphamide (CYP)-evoked OAB model in response to melatonin (MLT; antioxidant and MT receptor agonist) or agomelatine (AMT; MT receptor agonist and 5HT2C receptor antagonist).
Material/Methods: Seven groups were studied: 1 – control, 2-4 – MLT treated AOAB and COAB rats, 5-7 – AMT treated AOAB and COAB rats. AOAB model was evoked by single CYP administration (IP 200 mg/kg body weight), while COAB one was induced by a four-time administration of CYP (IP 75 mg/kg body weight). Each group underwent urethane anesthesia to perform urodynamic recordings in resting conditions and after administration 50 (group 2 or 5), 75 (group 3 or 6) or 100 mg/kg (group 4 or 7) of melatonin (groups 2-4) or agomelatine (groups 5-7), followed by classical urodynamic parameters assessment.
Results: Neither melatonin nor agomelatine did not affect urodynamic parameters in the AOAB rats. In COAB model, after 75 and 100 mg/kg of MLT we revealed an improvement in urodynamic parameters. AMT (75 and 100 mg/kg) administration caused deterioration of urodynamic findings suggesting bladder overactivity exacerbation.
Disscussion: In summary, melatonin ameliorates bladder overactivity in cyclophosphamide-induced COAB. Agomelatine, contrary to melatonin, aggravates bladder dysfunction in this group. These findings suggest that the improvement in urodynamic parameters after melatonin administration may be due to its antioxidative profile and is not related to MT receptors activation. However, agomelatine’s unfavorable action on the bladder, resulting in its overactivity in COAB group, may not only be the result of MT receptor activation without the concomitant antioxidative effects but may also occur secondarily to co-existing 5HT2C receptor antagonism.
Key words:overactive bladder (OAB) • urodynamic study • melatonin • agomelatine
List of abbreviations:
AMT – agomelatine; AOAB – acute overactive bladder; COAB – chronic overactive bladder; CYP – cyclophosphamide; DO – detrusor overactivity; HC – hemorrhagic cystitis; LUT – lower urinary tract; MLT – melatonin; OAB – overactive bladder.
Urodynamic parameters abbreviations:
PN – peak number; PNM – peak number per minute; ICI – intercontraction interval [s]; BP – basal pressure [cm H2O]; TP – threshold pressure [cm H2O]; MVP – micturition voiding pressure [cm H2O]; BC – bladder capacity [ml/cm H2O].
Introduction
The overactive bladder (OAB) was defined in 2002 by the International Continence Society as urinary urgency with or without urge incontinence, usually associated with frequency and nocturia, in the absence of proven pathological or metabolic disorders (such as: lower urinary tract (LUT) infection, bladder cancer, and benign prostatic enlargement) or other obvious pathology [11,12]. According to the latest terminology and 2006 definition update, OAB is characterized by urgency with or without urgency incontinence, usually with increased daytime frequency and nocturia [11]. This clinical entity occurs with global prevalence ranging from 8% to 16%, and varies between populations in relation to gender, age of responder and diagnostic criteria [11,36].
Pathogenesis of overactive bladder is complex and still not fully understood, though the two key theories that have been proposed implicate both neurogenic and myogenic factors. The neurogenic OAB development theory is regarded to be of essential meaning, suggesting both central and peripheral LUT innervation disturbances as main pathophysiological factors.
The pathophysiological description of this disease emphasizes dysfunction of the bladder innervation (afferent and efferent autonomic fibers as well as the involvement of central points). Undoubtedly, a crucial and final role in the pathogenesis of OAB play disturbances of bladder wall receptors’, the release of neurotransmitters acting upon these receptors, and local inflammatory process, which contributes through disturbed paracrine activity of urothelium, and results in hypersensitive efferent and afferent nerve fibers, and finally produces bladder dysmotility [1,22].
It is generally believed that contraction of the detrusor smooth muscle is a consequence of the activation of M1/M3 muscarinic receptors due to acetylcholine release from efferent nerve endings. There are also other receptor types in bladder, thus many chemicals released from the inflammatorily altered urothelium or delivered from systemic circulation may be involved in OAB development [1,11,16,22]. One of the agents which are able to affect bladder function is melatonin, and melatonin receptors have also been found in the bladder wall [8].
Melatonin (MLT), discovered in 1958 by Aaron Lerner et al. [6] is a hormone, secreted by pineal gland. For some time, MLT was regarded to be a physiologically useless hormone. However, studies conducted at the end of 1970s established that MLT is a hormone engaged in sleep wake cycle, secreted in inverse proportion to the length of diurnal and seasonal photoperiod interval [6,17]. However, MLT seems to produce numerous other effects that can also be observed in the lower urinary tract. Radioisotope studies revealed that MLT receptors (MT1/MT2) are situated in other, apart from hypothalamus, structures of the central nervous system, as well as in cardiovascular system (aorta, ventricles, coronary vessels), digestive tract (bile epithelium, duodenal enterocytes), genitourinary tract (bladder smooth muscles, ovarian cell granulosa layer, testicular epithelium) [8,17,25]. The MLT pharmacodynamic action is explained by four mechanisms: 1) the influence of MT receptors, 2) the activation of nuclear orphan ROR/RZS receptors, 3) the ability to bind to intracellular proteins (such as calmodulin), and 4) strong antioxidative effect (more pronounced than that determined for vitamin E). Hence, these are compelling reasons to presume that MLT might have beneficial action in diseases depended on oxidative stress, especially those that are neurodegenerative [15,33].
Contrary to the pleiotropic effects of MLT, agomelatine, the first synthetic MLT analogue with proven antidepressant potential, is MT1/MT2 agonist without antioxidant properties. At the same time, agomelatine is 5HT2C receptor antagonist and indirectly increases dopamine and noradrenaline levels [9,13,37].
Nevertheless, OAB is characterized by detrusor overactivity (DO) which is the main abnormality noted in urodynamic studies (bladder pressure recordings). The DO phenomenon can be explored using experimental OAB models. One of the best described and methodically developed is that of chemical cystitis induced by cyclophosphamide (CYP). This model, first proposed by Cox [7], is frequently used by other researches in this field, often with minor modifications.
The aim of the study was to investigate the influence of two pharmacologically active agents, melatonin and agomelatine, on bladder contractility in experimental, cyclophosphamide-induced overactive bladder model. As previously mentioned, urothelium with disturbed endocrine activity, such as that in OAB, releases various mediators, including reactive oxygen species, which contribute to bladder dysfunction. Hence, our aim was to investigate the effect of melatonin on urodynamic parameters. Moreover, in order to differentiate whether the potential effects of reducing DO are more dependent on the antioxidant action of melatonin, or are a result of interaction with the receptor, we used agomelatine – a mixed agonist of MT receptor and 5-HT antagonist that does not possess antioxidant activity.
Material and methods
Animals
The experiment was carried out using 70 female Wistar rats. The animals were obtained from the central laboratory. Upon the arrival at the animal house of Pathophysiology Department, the rats were placed five per cage and allowed to acclimatize for one week. The animals were housed in room temperature, with 12-12 hours day-night cycle, with standard food (Labofeed Kcynia) and freely available water. Cyclophosphamide (CYP), a nitrogen mustard derivative chemotherapeutic agent was injected IP to produce a model of chemically induced hemorrhagic cystitis (HC). Depending on the CYP dose, it is possible to induce both acute (AOAB) and chronic (COAB) overactive bladder models.
The study was performed in three models: 1) control rats (10 animals; mean body weight 273.3±36.0 g), 2) AOAB group (30 rats, mean body weight 306.8±30.4 g), and 3) COAB group (30 rats, mean body weight 289.3±42.1 g). The animals were selected to each group at random.
Chemicals
Cyclophosphamide (cyclophosphamide monohydrate), melatonin (N-acetyl-5-methoxytryptamine) and urethane (ethyl carbamate) were obtained from Sigma Aldrich. Agomelatine was used in form of commercial preparat (brand name Valdoxan 25mg, Servier).
Studied groups and experimental protocol
AOAB – Acute Overactive Bladder group
AOAB model was evoked by a single IP administration of cyclophosphamide (Sigma-Aldrich; 200 mg/kg body weight). According to literature [5,10], acute hemorrhagic cystitis (HC) with overactivity develops 4 to 24 hours after administration of CYP at previously mentioned dose. Indirect proof of the development of HC was hematuria observed in all rats. The next day, urodynamic recording was made before and after melatonin or agomelatine administration and then the rats were sacrificed by an overdose of pentobarbital (Morbital, Biowet Pulawy).
COAB – Chronic Overactive Bladder group
Model of chronic overactive bladder (COAB) was induced by a four-time IP administration of CYP (Sigma-Aldrich; 75 mg/kg body weight), administered every third day of the week (first, third, fifth and seventh day), resulting in a chronic chemical HC [5,10]. In this case hematuria was also regarded as the indirect evidence for the development of HC. This symptom was observed progressively in animals subjected to the CYP treatment, and present in almost all subjects after the last dose. On the eighth day of the experiment, similarly to AOAB rats, urodynamic recordings were performed before and after MLT or AMT administration, after which the animals were sacrificed as above.
Control group
Tested animals received IP injections of saline in a volume equivalent to doses of drugs used in AOAB/COAB groups. In control rats we took only resting urodynamic recordings as a comparison to those ones obtained in both OAB groups to ascertain if they really present bladder overactivity.
Finally, we distinguished seven studied groups
1 – control, 2-4 – AOAB/COAB rats that were given 50, 75 or 100mg/kg of melatonin (groups: 2,3,4; respectively) during urodynamic recordings and 5-7 – AOAB/COAB rats that were administered 50, 75 or 100mg/kg of agomelatine (groups: 5,6,7; respectively) during urodynamic studies.
Urodynamic studies
In each group, urodynamic recordings were performed under urethane anaesthesia (1.2 g/kg of body weight). Urethane was used after taking into consideration its relatively small potential for the impairment of the urinary bladder motility, as described previously [18,19]. In anaesthetized rat, the abdomen was opened through the low midline abdominal incision and the urinary bladder was exposed. The polyethylene catheter (external diameter 0.97 mm/internal diameter 0.58 mm, BALT Poland), connected to pressure transducer with analysis hardware (Power Lab; Chart 5 Pro v.5.4.2, ADInstruments) and injection pump (Unipan 340A), was inserted into the dome of the bladder through a small incision. The catheter was fixed in place with silk ligature 4-0. Cathetered bladders were left to stabilize for 15 minutes. To begin with, after system calibration, the baseline recordings were taken at room temperature during continuous saline infusion of 0.046 ml/min for 15 minutes. Then 50, 75 or 100 mg/kg of the studied agent (melatonin; Sigma Aldrich – in groups 2-4, or agomelatine; Valdoxan – in groups 5-7), dissolved previously in pure ethanol and diluted 1: 10 with saline, was administered IP, and the recording was continued for another 30 minutes. The values that were obtained during the study were subjected to analysis and calculation of standard urodynamic parameters: peak number (PN), peak number per minute (PNM), intercontraction interval (ICI [s]), basal pressure (BP [cm H2O]), threshold pressure (TP [cm H2O]), micturition voiding pressure (MVP [cm H2O]), and bladder capacity (BC [ml/cm H2O]). During the experiment the animals were kept under a heating lamp to prevent a fall in body temperature. Based on the literature reviewed, a dose of 50 or 75 or 100 mg/kg of MLT was administered IP (groups 2-4). Selection of the administered MLT dose was dictated by the review of the literature from different fields (experimental work in the field of neurology, gastroenterology). There are reports of intraperitoneal melatonin administered as a single high dose (100-200 mg/kg) [20,23,32] as well as the use of low but repeated doses (from below 1.0 to 50 mg/kg body weight) [30,31,32]. Consequently, we decided to use an intermediate dose to avoid both under- and overdosing of this compound. Because of scant data on the amounts of agomelatine (groups 5-7) routinely employed in the experimental work, we used a dose similar to melatonin. The number of the subgroup for the studied agent in the given dose and OAB model was 5 individuals, hence our results should be treated as preliminary ones.
Urinary bladder assessment
After urodynamic study, each animal was sacrificed with pentobarbital (Morbital, Biowet Puławy) overdose, the urodynamic catheter was taken out and the bladders were removed for histological and visual assessment. In both AOAB and COAB rats, urinary bladders were red, swollen and in selected cases covered by abundant serosal petechial suffusions. Leucocytic infiltration of the bladder wall was demonstrated in both groups of OAB. Histologically the inflammatory changes were more pronounced in COAB rats. Control rats had normal bladders.
Ethics
The study protocol was approved by the First Local Ethic Committee in Cracow (agreement decision 126/2010).
Statistical analysis
The results were displayed as mean ±SD. In both AOAB and COAB models, the intragroup differences in urodynamic parameters values before and after studied agent were estimated. Firstly, an initial statistical analysis was performed using non-parametric “signs” test to evaluate, whether urodynamic parameters calculated both before and after application of studied pharmacological agent differ between itself. This test is based on signs of differences among pairs of results (dependent variables) and enables quality comparing differences before and after applying of the selected drug. A null hypothesis telling that mean variations of the results in both analysed periods of the recordings are identical against the alternative H1 hypothesis assuming the existence of such differences was being verified. In the next step, proper statistical analysis was calculated with classical parametric t-Student test with p=0.05 or lower.
Results
The examples of resting urodynamic recordings obtained in both control (figure 1) and AOAB/COAB studied animals (figure 2) are given below. The control rats (group 1) demonstrated normal bladder activity, being an indirect evidence of bladder overactivity rejestrated in both AOAB/COAB models (groups 2-7).

Figure 1. The examples of urodynamic recordings obtained in control rats

Figure 2. The examples of urodynamic recordings obtained in OAB rats
Melatonin and AOAB/COAB models
In AOAB, melatonin in dose 50mg/kg (group 2) did not significantly affect any of the urodynamic parameters. The only observed change was PN increase (+31.1%) when 75 mg/kg of MLT was applied (group 3). 100mg/kg of melatonin (group 4) caused the increase of PN (+21.2%) and ICI (+29.9%). The other urodynamic parameters did not differ significantly in both the baseline and after MLT application periods of recording.
COAB group was characterized by only PNM (-27.3%) decrease (for MLT dose 50 mg/kg; group 2). When applying 75 mg/kg of MLT (group 3), PN (+61.6%), BP (+62.0%), MVP (+30.1%) and BC (+80.0%) increases were observed. After 100 mg/kg of MLT (group 4) we found PNM (-37.1%) decrease with ICI (+342.6%), MVP (+23.8%) and BC (+348.2%) increment.
Agomelatine and AOAB/COAB models
In AOAB, after 50mg/kg of agomelatine (group 5), the only observed change was BC decrease (-88.5%). After 75 and 100 mg/kg (groups 6 and 7, respectively), both PN (+21.8% and +21.2%) and ICI (+36.3% and +29.9%) increased, respectively.
COAB rats displayed only MVP increase (+21.1%) after 50 mg/kg of agomelatine (group 5). When administrating 75 mg/kg (group 6), we noted PN (+32.8%) increase, but with BP (-19.5%), TP (-21.7%), and MVP (-23.0%) decreases. Agomelatine in 100mg/kg (group 7) caused ICI (-45.2%) and MVP (-19.4%) lowering with PNM increase (+50%).
The results that were discussed briefly above are presented in tables 1 and 2 below (in numerical values).
Table 1. Urodynamic parameters in AOAB and COAB experimental models before and after melatonin administration
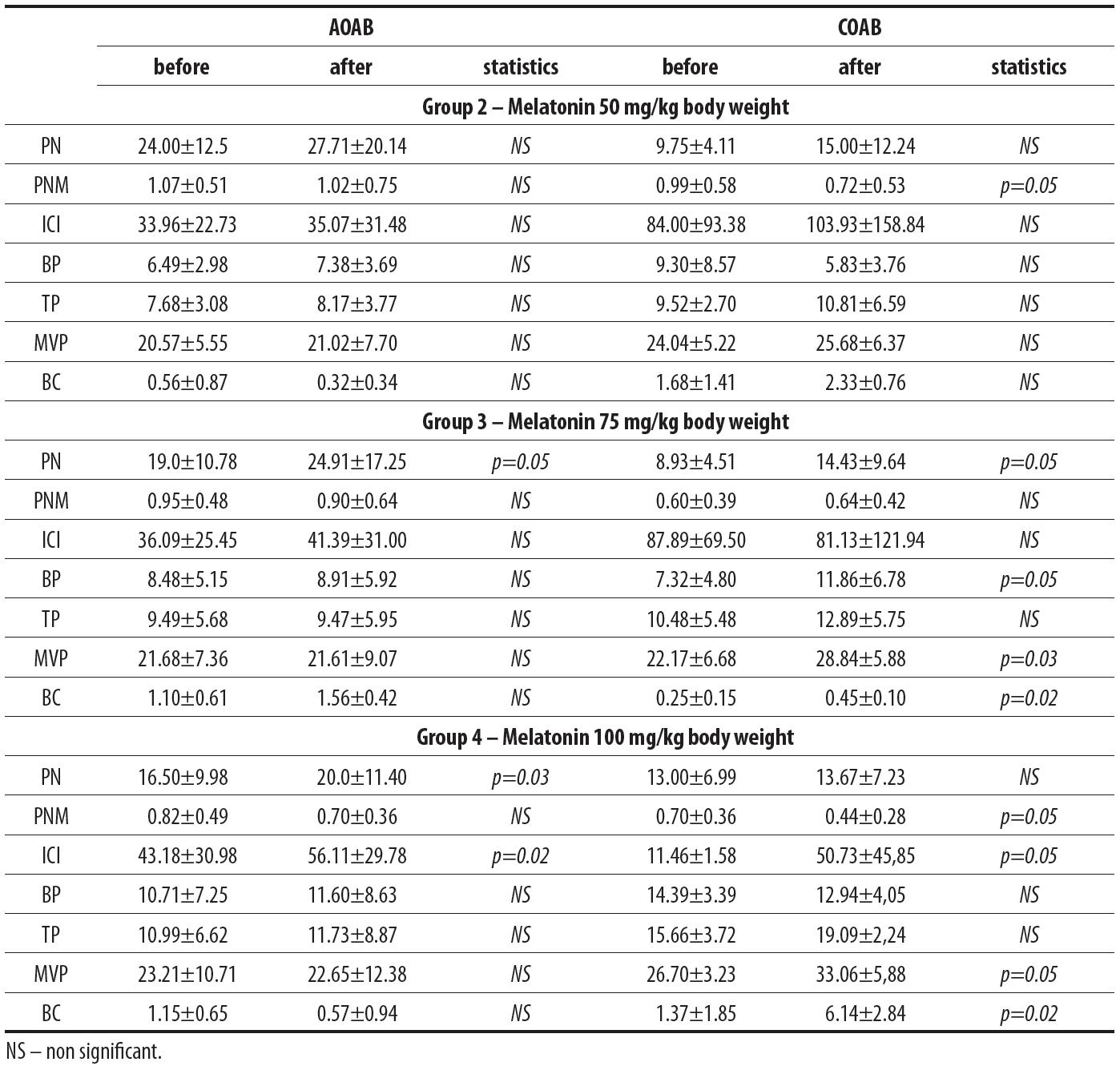
Table 2. Urodynamic parameters in AOAB and COAB experimental models before and after agomelatine administration

Disscussion
The key finding of our study is that MLT in higher doses (75 and 100 mg/kg) ameliorates bladder overreactivity in CYP-induced chronic OAB model (COAB). In urodynamic studies recorded in this group, there was observed a shift of threshold pressure towards a higher value together with an increase in bladder capacity. However, in acute OAB (AOAB) MLT did not alter bladder overactivity. Agomelatine, similarly to melatonin, was ineffective in AOAB improvement but contrary to melatonin, aggravated detrusor overactivity in COAB (in doses 75 and 100 mg/kg).
The literature reports relating to MLT’s and its analogues’ influence on bladder functioning are scant and mostly concerned with the histological and biochemical features of these compounds; drawing conclusions about bladder motility only indirectly. Topal et al. [34] studied the NO synthase (iNOS) activity and ROS level after MLT administration of 5 or 10 mg/kg, using a model similar to our OAB model that was induced by 100 mg/kg of CYP. They demonstrated that according to theoretical expectations described above, MLT decreased iNOS activity and oxidative stress resulting in HC symptoms appeasement. Our results partly confirm their conclusions, but in relation to CYP dose of 75 mg/kg applied four times during a week. Higher CYP dose, 200 mg/kg, which was used to evoke AOAB, did not diminish bladder contractility. In our opinion this is a consequence of critical HC development that proceeds with activation of numerous mediators aside from ROS, thus antioxidants are not essential in amelioration of this pathophysiological condition.
Tripathi et al. [35] continued Topal et al. [34] study by attempting to pinpoint MLT’s protective mechanism. They found that MLT induced an increase in Nrf2 and NF-κB factors. These agents stimulate the gene responsible for the expression of antioxidative enzymes, the aim of current search for new chemopreventive agents. The beneficial antioxidative and indirectly DO ameliorating effect of MLT, resulting from its pleiotropic properties, was also demonstrated by Sadir et al. [26]. They revealed that MLT added to Mesna (a “classic” drug used in patients receiving CYP), augmented chemopreventive effect and lessened bladder injury. Hence, taking into consideration our findings, it seems that the results are dependent on CYP dose – in chronic treatment both MLT and Mesna display a beneficial role, but after application of a single urotoxic CYP dose, MLT did not produce the desired effect. It is worth remembering that antioxidative properties of MLT, associated with morphological and functional features of the bladder, were also demonstrated in other experimental models of OAB: protamine sulphate-induced [4], chronic water avoidance stress [3], postreperfusive [29], radiation-induced bladder injury [28], and in partial obstructive OAB model [24].
In summary, there are numerous well documented studies confirming the beneficial role of MLT in reducing the intensity of bladder inflammation by antioxidative mechanisms and thus indirectly improving bladder functioning. A few studies directly investigated bladder motility changes after MLT administration. Semercioz et al. [27] evaluated the contractility of guinea pig bladder fragments via in vitro conditioning of hyperreactivity (tests in aerated, thermostable buffered solutions with pH=7.4 and in the presence of KCl or acetylcholine). Addition of MLT (100 µmol/l and 300 µmol/l) to such a medium caused a decrease in the amplitude of contraction (this parameter is equivalent to MVP in our study). Moreover, MLT caused a decrease in the frequency of the contractions during 10 minute recording (this finding corresponds to PMN in our study) when KCl was applied, but exerted no influence on acetylcholine. An interesting study was also conducted by Matsuta et al. [21] who analyzed the effects of MLT and bicucculine (GABA-A receptor antagonist) interventricular administration on the bladder. Matsuta et al. [21] assumed that orthotopic, centrally secreted MLT, may produce inhibition of the micturition centers (and might explain the beneficial effect of MLT in reducing nocturia in some patients) via GABA-ergic system. They revealed that the more centrally MLT dose was applied, the more augmentation of the bladder capacity (without micturition voiding pressure) was observed. When bicucculin was administered together with MLT, the effects mentioned above were abolished, thus suggesting that MLT works by indirect activation of GABA receptors [21]. In our opinion, this study deserves special attention because when the conclusions of our study are taken into consideration, it may be suspected that when MLT is administrated peripherally it acts mostly as an antioxidant with the predominance of mechanisms that are not originating within the receptor.
A study by Gomez-Pinilla et al. [14] used methodology similar to ours when they investigated bladder overactivity developed in the process of aging (and as a consequence – in advanced oxidative stress) in young and senile guinea pigs treated with MLT per os (2.5 mg/kg) for 21 days. They demonstrated that urodynamic recordings made in control senile animals were characterized by increased spontaneous (not associated with bladder emptying) contractions noted in inter-miction periods, as well as a decrease in storage time, micturition pressure and bladder capacity. These findings meet OAB criteria, described in both animal OAB model and in clinical conditions. The animals treated with MLT displayed urodynamic parameters improvement, reaching similar values as those observed in young, healthy population. Thus, MLT, according to Gomez-Pinilla et al. [14] by lowering oxidative stress that becomes augmented during aging, reverses unfavorable bladder dysmotility. In our opinion, despite many differences in the study protocol (route of administration and dose of MLT) and general methodology (physiological OAB related to aging vs. CYP-induced OAB model), the Gomez-Pinilla et al. study [14] may be compared somewhat to our COAB population. Once again, Gomez-Pinilla et al. [14] conclusions would support our hypothesis of beneficial melatonin effect in COAB.
However, we must emphasize, that it is difficult to compare our results directly to previously mentioned studies while taking into account the methodological differences (OAB model, MLT route of administration and dose). Unfortunately, there is a lack of studies reproducing our experimental conditions, thus we can only compare our findings to similar citations. We used 200 mg/kg of CYP to induce AOAB model (in accordance with other researchers [2,5,10]); while studies discussed above [26,34,35] were based on the administration of 100-150 mg/kg of CYP. This must have resulted in an escalated HC (and as a consequence in a more intense overactivity of the bladder) development than in our study. Moreover, another crucial difference was that contrary to others researchers we administered MLT during urodynamic studies, and not in the preceding period. Thus, the effects that were observed by us had short-term character. Apart from these limitations, our experiment confirms the hypothesis that MLT has an alleviating influence on bladder overactivity (proven in COAB condition).
In our study we tried to evaluate the functioning of the bladder altered by inflammation after administration of MLT, assuming that observed effects may result from both the antioxidative properties of MLT mentioned above, and MT receptors excitation. To differentiate this, we also estimated urodynamic recordings after administration of agomelatine, a MT receptor agonist with no antioxidative properties. The results obtained after agomelatine injection suggest that contrary to MLT, no beneficial effect in terms of diminishing DO in COAB rats was found (in fact, even more pronounced overactivity characteristics were observed). On the one hand, the disadvantageous impact of agomelatine on bladder contractility may confirm the hypothesis that MLT improves bladder functioning in COAB by antioxidative mechanisms mostly and not through interaction with the receptor. On the other hand; however, this findings may be secondary to the concurrent antagonistic influence of agomelatine on 5HT2C receptors. Possibly, the serotoninergic receptors blockade abolishes the potential beneficial activation of MT receptors, multiplying in this way the antioxidative mechanisms. Unfortunately, to our knowledge, there are no studies with clinical and experimental estimation of the influence of agomelatine on the bladder functioning in OAB. Thus, we are not in a position to compare our results with the conclusions of other studies. It seems that this area of research, concerned with searching for new pharmacologically active OAB agents, needs further studies to establish grounds for interchangeably evaluating our observations.
In summary, MLT decreased the intensity of bladder overactivity in experimental chronic, CYP-induced overactive bladder model (COAB). In acute model, (AOAB), associated with development of severe hemorrhagic cystitis, MLT was ineffective in ameliorating bladder overactivity.
Agomelatine, similarly to melatonin, was inactive in AOAB, but contrary to MLT, aggravated bladder overactivity in COAB model.
In our opinion, these findings suggest that urodynamic improvement after MLT in COAB group resulted from its antioxidative capacity, and were not associated with MT receptor activation. It is possible that agomelatine-induced exacerbation of bladder overactivity in COAB is related to the antagonistic action affecting the 5HT2C receptors, and is not connected to the MT receptors activation or its lack of antioxidative capacity. This issue needs further exploration using selective agents that act on the 5HT2C receptors.
REFERENCES
[1] Andersson K.E., Pehrson R.: CNS involvement in overactive bladder. Pathophysiology and opportunities for pharmacological intervention. Drugs, 2003; 63: 2595-2611
[PubMed]
[2] Boucher M., Meen M., Cordon J.P., Coudore F., Kemeny J.L., Eschalier A.: Cyclophosphamide-induced cystitis in freely-moving conscious rats: behavioral approach to a new model of visceral pain. J. Urol., 2000; 164: 203-208
[PubMed]
[3] Cetinel S., Ercan F., Cikler E., Contuk G., Sener G.: Protective effect of melatonin on water avoidance stress induced degeneration of the bladder. J. Urol., 2005; 173: 267-270
[PubMed]
[4] Cetinel S., Ercan F., Sirvanci S., Sehirli O., Ersoy Y., San T., Sener G.: The ameliorating effect of melatonin on protamine sulfate induced bladder injury and its relationship to interstitial cystitis. J. Urol., 2003; 169: 1564-1568
[PubMed]
[5] Chopra B., Barrick S.R., Meyers S., Beckel J.M., Zeidel M.L., Ford A.P., de Groat W.C., Birder L.A.: Expression and function of bradykinin B1 and B2 receptors in normal and inflamed rat urinary bladder urothelium. J. Physiol. 2005; 562: 859-871
[PubMed] [Full Text HTML] [Full Text PDF]
[6] Claustrat B., Brun J., Chazot G.: The basic physiology and pathophysiology of melatonin. Sleep Med. Rev., 2005; 9: 11-24
[PubMed]
[7] Cox P.J.: Cyclophosphamide cystitis – identification of acroleine as the causative agent. Biochem. Pharmacol., 1979; 28: 2045-2049
[PubMed]
[8] Danielczyk K., Dzięgiel P.: Receptory melatoninowe oraz ich rola w onkostatycznym działaniu melatoniny. Postępy Hig. Med. Dośw., 2009; 63: 425-434
[PubMed] [Full Text HTML] [Full Text PDF]
[9] de Bodinat C., Guardiola-Lemaitre B., Mocaer E., Renard P., Munoz C., Millan M.J.: Agomelatine, the first melatonergic antidepressant: discovery, characterization and development. Nat. Rev. Drug. Discov., 2010; 9: 628-642
[PubMed]
[10] Dinis P., Churrua A., Avelino A., Yaqoob M., Bevan S., Nagy I., Cruz F.: Anandamide-evoked activation of vanilloid receptor 1 contributes to the development of bladder hyperreflexia and nociceptive transmission to spinal dorsal horn neurons in cystitis. J. Neurosci., 2004; 24: 11253-11263
[PubMed] [Full Text HTML] [Full Text PDF]
[11] Dobrek Ł., Juszczak K., Wyczółkowski M., Thor P.J.: Overactive bladder – current definition and basic pathophysiological concepts. Adv. Clin. Exp. Med., 2011; 20: 119-129
[12] Futyma K., Rechberger T.: Nowe opcje terapeutyczne w leczeniu nadaktywnego pecherza moczowego. Przegl. Urol., 2008; 9(6): 27-29
[Full Text HTML]
[13] Girish M.B., Bhuvana K., Nagesh Raju G., Sarala N.: A novel atypical antidepressant drug: agomelatine – a review. Int. J. Pharm. Biomed. Res., 2010; 1: 113-116
[14] Gomez-Pinilla P.J., Gomez M.F., Sward K., Hedlund P., Hellstrand P., Camello P.J., Andersson K.E., Pozo M.J.: Melatonin restores impaired contractility in aged guinea pig urinary bladder. J. Pineal Res., 2008; 44: 416-425
[PubMed]
[15] Hardeland R.: Antioxidative protection by melatonin: multiplicity of mechanisms from radical detoxification to radical avoidance. Endocrine, 2005; 27: 119-130
[PubMed]
[16] Hashim H., Abrams P.: Overactive bladder: an update. Curr. Opin. Urol., 2007; 17: 231-236
[PubMed]
[17] Karasek M., Winczyk K.: Melatonin in humans. J. Physiol. Pharmacol., 2006; 57 (Suppl. 5): 19-39
[PubMed] [Full Text PDF]
[18] Maggi C.A., Meli A.: Suitability of urethane anesthesia for physiopharmacological investigations in various systems. Part 1: general considerations. Experientia, 1986; 42: 109-114
[PubMed]
[19] Maggi C.A., Meli A.: Suitability of urethane anesthesia for physiopharmacological investigations in various systems. Part 3: Other systems and conclusions. Experientia, 1986; 42: 531-537
[PubMed]
[20] Mantovani M., Kaster M.P., Pertile R., Calixto J.B., Rodrigues A.L., Santos A.R.: Mechanisms involved in the antinociception caused by melatonin in mice. J. Pineal Res., 2006; 41: 382-389
[PubMed]
[21] Matsuta Y., Yusup A., Tanase K., Ishida H., Akino H., Yokoyama O.: Melatonin increases bladder capacity via GABAergic system and decreases urine volume in rats. J. Urol., 2010; 184: 386-391
[PubMed]
[22] Moore C.K., Goldman H.B.: The bladder epithelium and overactive bladder: what we know. Curr. Urol. Rep., 2006; 7: 447-449
[PubMed]
[23] Naguib M., Schmid P.G.3rd, Baker M.T.: The electroencephalographic effects of IV anaesthetic doses of melatonin: comparative studies with thiopental and propofol. Anaesth. Analg., 2003; 97: 238-243
[PubMed] [Full Text HTML] [Full Text PDF]
[24] Onur R., Tasdemir C., Seckin D., Ilhan N., Kutlu S., Akpolat N.: Combined use of melatonin and terazosin restores bladder contractility in rabbits with partial outlet obstruction. Urology, 2008; 72: 439-443
[PubMed]
[25] Pandi-Perumal S.R., Trakht I., Srinivasan V., Spence D.W., Maestroni G.J., Zisapel N., Cardinali D.P.: Physiological effects of melatonin: role of melatonin receptors and signal transduction pathways. Prog. Neurobiol., 2008; 85: 335-353
[PubMed]
[26] Sadir S., Deveci S., Korkmaz A., Oter S.: Alpha-tocopherol, beta-carotene and melatonin administration protects cyclophosphamide-induced oxidative damage to bladder tissue in rats. Cell. Biochem. Funct., 2007; 25: 521-526
[PubMed]
[27] Semercioz A., Onur R., Ayar A., Orhan I.: The inhibitory role of melatonin on isolated guinea-pig urinary bladder: an endogenous hormone effect. BJU Int., 2004; 94: 1373-1376
[PubMed]
[28] Sener G., Atasoy B.M., Ersoy Y., Arbak S., Sengoz M., Yegen B.C.: Melatonin protects against ionizing radiation-induced oxidative damage in corpus cavernosum and urinary bladder in rats. J. Pineal Res., 2004; 37: 241-246
[PubMed]
[29] Sener G., Sehirli A., Paskaloglu K., Dulger G., Alican I.: Melatonin treatment protects against ischemia/reperfusion-induced functional and biochemical changes in rat urinary bladder. J. Pineal Res., 2003; 34: 226-230
[PubMed]
[30] Shaker M.E., Houssen M.E., Abo-Hashem E.M., Ibrahim T.M.: Comparison of vitamin E, L-carnitine and melatonin in ameliorating carbon tetrachloride and diabetes induced hepatic oxidative stress. J. Physiol. Biochem., 2009; 65: 225-233
[PubMed]
[31] Srivastava A.K., Gupta S.K., Jain S., Gupta Y.K.: Effect of melatonin and phenytoin on an intracortical ferric chloride model of posttraumatic seizures in rats. Methods Find. Exp. Clin. Pharmacol., 2002; 24: 145-149
[PubMed]
[32] Sugden D.: Psychopharmacological effects of melatonin in mouse and rat. J. Pharmacol. Exp. Ther., 1983; 227: 587-591
[PubMed]
[33] Suzen S.: Recent developments of melatonin related antioxidant compounds. Comb. Chem. High Throughput Screen, 2006; 9: 409-419
[PubMed]
[34] Topal T., Oztas Y., Korkmaz A., Sadir S., Oter S., Coskun O., Bilgic H.: Melatonin ameliorates bladder damage induced by cyclophosphamide in rats. J. Pineal Res., 2005; 38: 272-277
[PubMed]
[35] Tripathi D.N., Jena G.B.: Effect of melatonin on the expression of Nrf2 and NF-κB during cyclophosphamide-induced urinary bladder injury in rat. J. Pineal Res., 2010; 48: 324-331
[PubMed]
[36] Tubaro A., Palleschi G.: Overactive bladder: epidemiology and social impact. Curr. Opin. Obstet. Gynecol., 2005; 17: 507-511
[PubMed]
[37] Zupancic M., Guilleminault C.: Agomelatine – a preliminary review of a new antidepressant. CNS Drugs, 2006; 20: 981-992
[PubMed]
The authors have no potential conflicts of interest to declare.